
Working on Wellness: The Rural Health and Employment Link
The relationship between health and employment is bidirectional and intensified by structural and geographic factors unique to rural communities.
Econ Focus
First/Second Quarter 2026
Adverse health events can be disruptive to employment. A health shock, such as suffering an injury or developing a chronic condition, can limit an individual's ability to perform the physical and mental demands of work, potentially leading to lower productivity, fewer hours, and even a labor force exit. But the relationship between health and employment doesn't end there — employment outcomes also influence health outcomes. Employment is a key social determinant of health, supporting well-being through financial stability and access to employer-provided health insurance. For some, workplace conditions can increase individual exposure to health risks.
In the Fifth District, the disparity in employment outcomes along the rural-urban continuum may be in part due to variation in health outcomes. Rural counties in the Fifth District on average have lower employment-to-population ratios compared to their urban counterparts. Rural counties also have poorer health outcomes compared to urban areas, including higher incidence of some chronic conditions, lower scores on self-reported measures of health, and lower life expectancy. The relationship between poor health and employment outcomes is consistent across geographies. However, features of rural places in particular — like greater distances between residents and amenities, lower population density, and industry and occupation characteristics — may exacerbate the incidence and severity of adverse health events and compound the negative relationship between poor health and employment. Recognizing the inherent challenges rural areas might face, communities across the Fifth District are looking for ways to ensure that high-quality health care, including preventative care, is available to all residents.
Rural-Urban Disparities in Employment
Differences in employment-to-population ratios and labor force participation rates along the rural-urban continuum suggest an underutilization of labor in some rural areas in the Fifth District. (See chart.) In 2023, the aggregated employment-to-population ratio was 64 percent in the most urban counties compared to 44 percent in the most rural counties in the District. The age composition of the population partially explains this difference, as rural areas tend to have a higher share of older adults who are more likely to be retired. But prime age (aged 25-54) labor force participation rates are also lower on average in rural counties. The prime age labor force participation rate varies from 87 percent for the most urban counties, to 69 percent for the most rural counties.
Poorer health outcomes in rural areas may partially explain this difference. According to a 2024 article in Systematic Reviews of the impact of health shocks on labor supply by Ken Chamuva Shawa of the International Labour Organization, Bruce Hollingsworth of Lancaster University, and Eugenio Zucchelli of AESARA, there is overwhelming evidence that poor health has a negative impact on labor supply. A 2019 report from the Urban Institute showed that workers who experienced a health shock were nearly 22 percentage points more likely to exit the labor force compared with all workers. Additionally, worse employment outcomes in rural areas may reinforce poor health outcomes and create a negative feedback loop. A 2021 American Journal of Industrial Medicine article by Sharon Silver and Jia Li of the Centers for Disease Control and Prevention and Brian Quay of the National Institutes of Health suggested that negative health outcomes increase as unemployment duration increases.
Rural-Urban Disparities in Health Outcomes
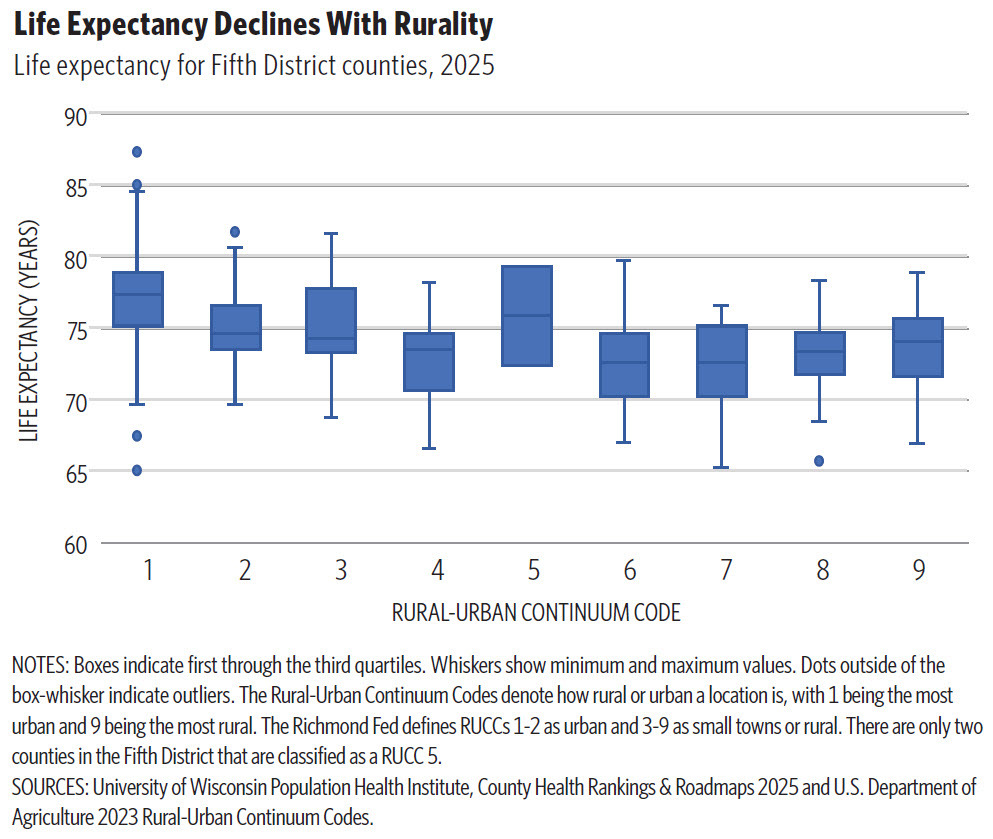
Health outcomes across several domains are worse in rural areas compared to their urban counterparts. One of the broadest measures of aggregate health at the regional level is life expectancy at birth, which measures the average lifespan of a newborn under current mortality conditions. In Fifth District states, median life expectancy is roughly three to four years higher in urban counties compared to the most rural counties. (See chart.) However, there is a wide distribution of outcomes within urban and rural spaces. Petersburg, Va., Hopewell, Va., and Chester County, S.C., severely underperform relative to the urban median, while some rural counties outperform their urban counter parts. Another indicator that provides a baseline measure of health from birth is low birth weight — a health metric associated with a variety of negative outcomes, including lower educational attainment, lower employment, and decreased earnings. The percentage of babies born with low birth weight is higher in rural Fifth District counties on average.
Self-reported healthy (or unhealthy) days are another health metric that reveal rural-urban health differences. This indicator measures the number of days that an individual reports feeling physically or mentally unwell during a 30-day period. Although self-reporting can be subjective, it is still a valuable tool for understanding how individuals view their health and ability to work. Indeed, the measure is connected to work: A 2004 article in the American Journal of Epidemiology and Community Health showed that counties with higher average unhealthy days also tend to have higher levels of unemployment, lower educational attainment, and higher prevalence of disability. In general, rural counties show slightly higher average unhealthy days compared to urban areas.
Why might rural counties have lower life expectancy or more unhealthy days? For one thing, chronic diseases like arthritis, hypertension, and diabetes are more prevalent in rural places, as are risk factors for long-term health problems, such as smoking and obesity. According to a 2017 report from the Centers for Disease Control and Prevention, accidental deaths from injuries, traffic accidents, and drug overdoses were 50 percent higher in rural areas. The opioid epidemic has been especially damaging to rural areas. A 2020 Rural Sociology article by David Peters and Andrew Hochstetler of Iowa State University, Shannon Monnat of Syracuse University, and Mark Berg of the University of Iowa found that most U.S. counties facing a prescription opioid epidemic are rural or nonmetropolitan. Rates of death due to opioid overdose are highest in the Appalachian region of the United States, and West Virginia consistently has the highest rate of opioid overdoses in the country.
Also, rates of self-reported disability are higher in many rural areas relative to urban areas. The Census Bureau's disability assessment covers a range of illnesses and conditions including vision, hearing, cognitive, independent living, ambulatory, and self-care limitations. In the Fifth District, self-reported rates of disability generally increase as rurality increases, though the largest disparity exists for older adults. (See charts.)
The link between a health shock and labor force exit often operates through the disability channel. Workers who suffer a health shock that creates work limitations can receive Social Security Disability Insurance (SSDI), which is typically available to workers with sufficient and recent work history. Some SSDI recipients also receive Supplemental Security Income (SSI), which is available to disabled persons of any age who either have no income or have limited financial resources. While some recipients of SSDI still work, there is evidence that the receipt of disability benefits provides a disincentive to work and tends to reduce labor supply. However, not all workers who exit the labor force due to a self-reported disability will pursue or qualify for federal benefits.
Rural-Specific Challenge Affecting Health
There are rural-specific challenges that can increase the occurrence of adverse health events, hinder their effective treatment, and negatively impact employment outcomes.
In the Fifth District, rural counties have higher poverty rates compared to urban counties. According to 2020 American Community Survey data, 47 percent of Fifth District rural counties had poverty rates above 17 percent, compared to 15 percent in urban counties. Fewer financial resources limit access to medical care — including preventative and routine visits, access to medication and treatment for minor or chronic health conditions, and access to healthy food. Educational attainment is also lower in rural areas. Higher levels of education are correlated with increased likelihood of employment, higher income, and better health outcomes. Additionally, more educated workers may have an advantage after an adverse health event: In a 2016 article in Labour Economics, Matthew Hill of the University of Southern California, Nicole Maestas of Harvard University, and Kathleen Mullen of the RAND Corporation found that workers who have at least some college education are 8 percentage points to 12 percentage points more likely than those with less than a high school education to receive employer accommodations that allow them to remain on the job following the onset of a new disability.
Lower population densities in rural areas often mean that residents must travel longer distances to access care, especially for specialized services that are not offered at nearby rural hospitals. According to a 2021 policy brief from the Southwest Rural Health Research Center of Texas A&M University, rural residents traveled over twice the distance of urban residents to receive medical or dental care. Lack of transportation can result in delays in the diagnoses of serious medical conditions and inconsistent treatment for chronic conditions. Transportation barriers can also hinder behaviors that support a healthy lifestyle, such as healthy eating and physical activity. Research suggests that rural residents have less access to healthy food due to higher costs and greater distances to supermarkets. Also, environmental and infrastructure limitations of rural areas, including less walkability and fewer parks and recreational spaces, can limit opportunities for physical activity.

Related Listening
In the April 15, 2026 episode of the Speaking of the Economy podcast, Surekha Carpenter and Bethany Greene discuss the connections between the health of workers and the health of labor markets in rural communities.
Some rural communities lack critical medical services, creating an environment where residents are medically underserved and may face higher rates of untreated chronic conditions and mortality. Also, rural hospitals face a unique set of financial challenges that impact their provision of services and increase their vulnerability to closure or consolidation. Low patient volumes compress margins, making it increasingly difficult to cover fixed costs. Additionally, due to higher levels of poverty and lower levels of employment in rural areas, a higher share of rural patients is either uninsured or using government health insurance programs like Medicaid and Medicare, resulting in lower reimbursement rates and higher instances of uncompensated care. According to a report from KFF, a nonprofit health policy organization, 44 percent of rural hospitals operated on negative margins in 2023, compared to 35 percent of urban hospitals.
With these financial challenges, some rural hospitals face difficult choices regarding the continuation of critical services that are less profitable, such as maternal health. According to a 2024 JAMA article the share of rural hospitals that had obstetric services declined from 57 percent to 48 percent between 2010 and 2022. And for other hospitals, financial challenges led to closure. According to the UNC Chapel Hill Rural Health Research Program, 22 rural hospitals in the Fifth District closed over the last two decades. Also, a 2026 report from The Commonwealth Fund, a foundation that promote health care improvements, shows that more than 20 percent of rural hospitals are currently at risk of closure.
Our Related Research
"Digital Access Deficiencies in Rural Health Care Deserts: Identifying a Role for Telehealth," Regional Matters, October 2024.
"The Role of Manufacturing in the Rural Fifth District," Regional Matters, April 2022.
"Why are Rural Hospitals Closing?" Regional Matters, October 2019.
Difficulty recruiting and retaining health care workers in rural areas presents another major challenge for rural residents accessing medical care. Nearly all rural counties in the Fifth District are classified as full or partial Health Professional Shortage Areas for mental health care, primary care, or dental care. The shortage of primary care professionals is particularly concerning as they serve as an entry point to health care and are essential for administering preventative care. There is also evidence that health systems that prioritize primary care have healthier populations. According to the Rural Health Information Hub, there are 5.1 primary care physicians per 10,000 people in rural areas compared to 7.9 in urban areas. In addition to primary care physicians, rural areas also lack other vital health care professionals such as nurses, mental health professionals, and specialists.
Structural issues that are unique to rural areas such as fewer housing options than in cities, limited job opportunities for spouses, lack of child care facilities, and lower salaries create barriers to the recruitment and retention of health care professionals. Additionally, there is evidence that the COVID-19 pandemic exacerbated rural workforce challenges. A 2022 National Rural Health Association policy brief reported that during the pandemic, many health care workers left rural settings for higher-paying opportunities. Rural hospitals, which have fewer financial resources, were unable to counter these incentives and retain staff who were in high demand.
Rural Labor Market Characteristics
The industry and occupational composition of many rural areas may also create work barriers for individuals with certain health conditions. For example, jobs with significant physical requirements may not accommodate an individual who develops mobility issues associated with a chronic health condition or injury. In fact, data on work activities from the U.S. Department of Labor's Occupational Information Network (O*NET) reveal that workers in nonmetro areas are more likely to be employed in roles that require performing general physical activities. O*NET defines such jobs as those involving "activities that require considerable use of your arms and legs and moving your whole body, such as climbing, lifting, balancing, walking, stooping and handling materials." The O*NET database assigns each occupation a score out of 100 that reflects the degree to which physical or manual work activities are performed. For example, electrical power line installers have a score of 90, indicating a high degree of job-related physical activities, while web developers have a score of 6. Using the occupational composition of an area's employment, it is possible to calculate a weighted average score for general physical job activity by region.
In all Fifth District states, nonmetro regions had higher general physical activity scores, which reveals that there is a larger share of employment opportunities that require a high level of physical activity. Additionally, workers in rural areas have more expo sure to hazardous conditions that can impact health outcomes. O*NET provides data that measure an occupation's level of exposure to hazardous equipment and hazardous conditions, which can be used to construct a weighted average score based on an area's occupational composition. The results show that workers in nonmetro areas are more exposed to hazardous work conditions and equipment, which may lead to a higher risk of injuries and other health conditions. (See charts.)
As previously mentioned, self-reported levels of disability are higher in rural areas compared to urban areas. There is a lack of data to show rural-urban differences in SSDI participation rates, but self-reported disability is associated with increased uptake of SSDI. While higher rates of self-reported disability and potentially higher rates of SSDI reflect disparities in access to health care, they may also reflect disparities in accommodative job opportunities and higher occupational risk. A 2016 Journal of Labor Economics article by Andreas Mueller of the University of Zurich, Jesse Rothstein of the University of California, Berkeley, and Till von Wachter of the University of California Los Angeles showed that SSDI awards increase during recessions, an indication that uptake in disability insurance may also be tied to local labor market conditions. Rural workers may have an increased likelihood of receiving disability because their ability to find gainful employment or make an occupational shift may be more limited than urban workers. As such, SSDI may play a unique role as a source of income stability in rural labor markets where employment is more concentrated in physically demanding and hazardous roles and alternative job opportunities are more limited.
Addressing Rural Health And Employment Challenges
Rural areas have concentrations of employment that are more likely to result in injury, and it can be difficult to access health care. So, what are rural communities doing to address those challenges? Many have focused on increasing access to health care and addressing the underlying determinants of health. To overcome shortages of health care facilities and the distances between residents and health amenities, many places have turned to improving telehealth services. While telehealth removes the physical distance between individuals and health care providers, it is dependent on the availability of reliable internet services. As such, broadband expansion and adoption, which many rural places have also struggled with, is a critical component to this solution. These improvements in technology infrastructure also serve to expand remote work access to rural residents, which can be accommodative for those with physically limiting health conditions.
Another way rural areas have addressed distance and transportation challenges is by offering flexible health care that meets people where they are. Marshall University's Marco Mobile Medicine, for example, aims to bring advanced health care, like early disease detection and chronic condition management, to rural West Virginians. Universities and community colleges often offer discounted or free services — achieving both workforce training for students and bridging the gap in health care access for low-income or uninsured residents.
Other solutions target the health and employment link explicitly. Employer-based initiatives, like on-site medical services for employees, can be especially valuable for hourly employees who otherwise would have to leave work and travel long distances to receive medical care.
Addressing the underlying determinants of health goes beyond just access. Some rural communities are now emphasizing multifaceted development aimed at improving the overall quality of a place, rather than addressing health in a vacuum. For example, Paola Gutiérrez of the South Carolina Office of Rural Health highlights initiatives that stress the importance of strengthening rural identity and promoting community engagement. Whether it be the creation of a new trail or a Main Street revitalization project, these initiatives help to retain residents by strengthening the physical and social environments that people live in. One example is the Purpose Built Communities model, which focuses on developing community vibrancy alongside economic vitality (including improving housing and education-to-career pathways).
The determinants of better health and employment outcomes are wide ranging and interconnected. Alongside immediate improvements to health care access, longer-term investments in quality of life can strengthen community morale, improve living environments, and make rural places attractive for residents and employers.
Subscribe to Econ Focus
Receive an email notification when Econ Focus is posted online.
By submitting this form you agree to the Bank's Terms & Conditions and Privacy Notice.
Contact Us